Printable Medical History Form For Dental Office
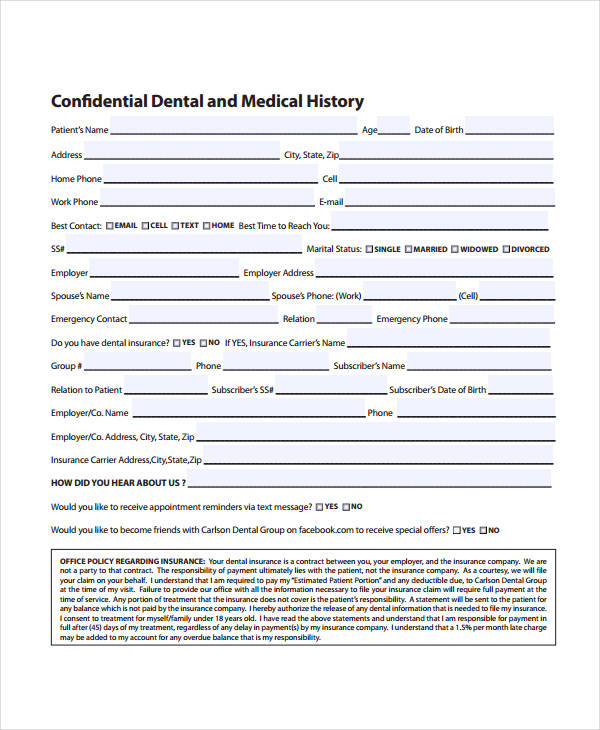
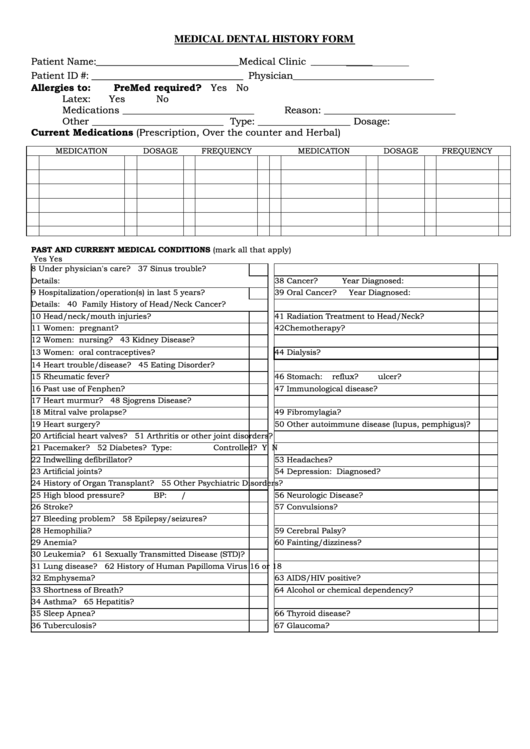
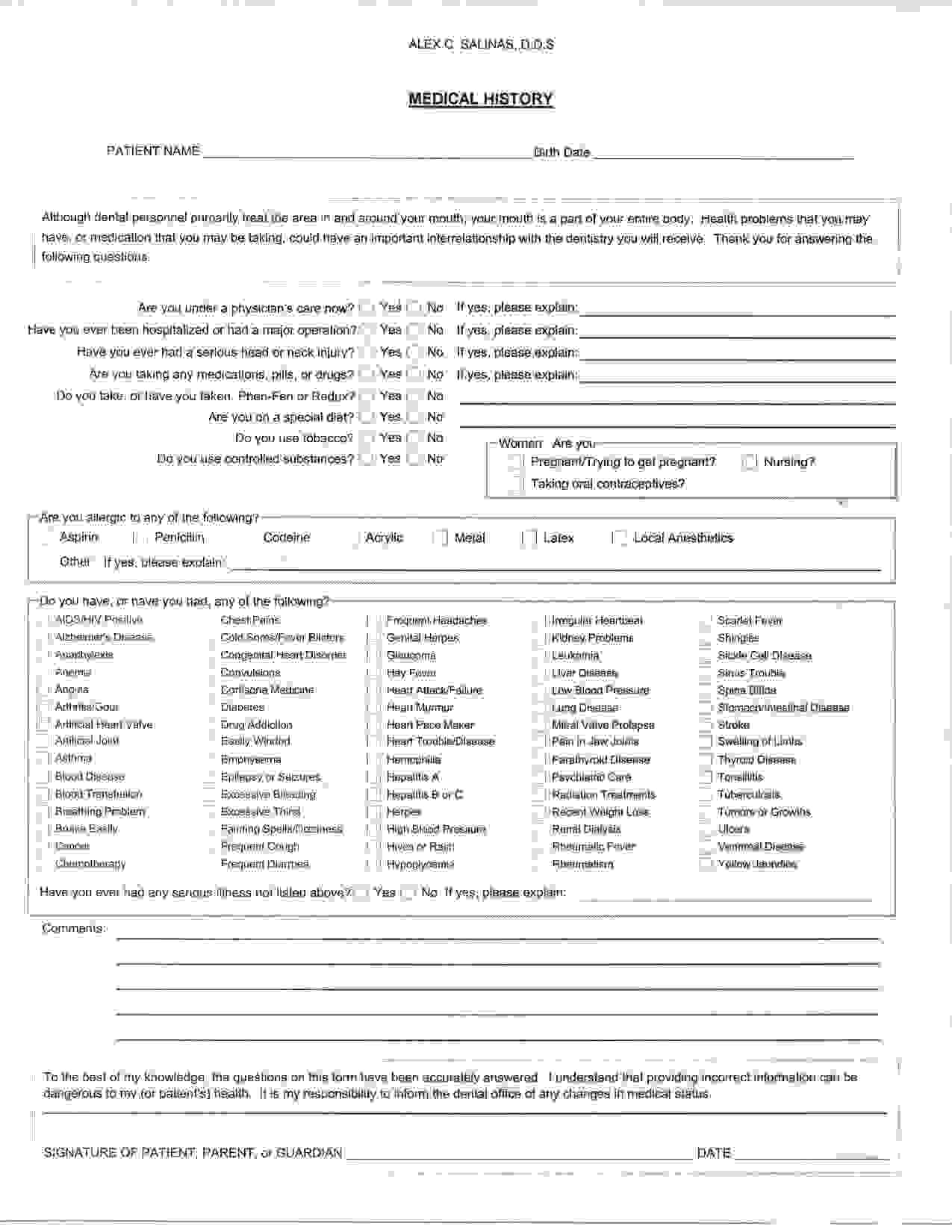
Printable Medical History Form For Dental Office - The following information is required to enable us to provide you with the best possible dental care. 89 treatment for periodontal (gum) disease? Date of your last dental exam: Current dental terminology © 2020 american dental association. What was done at that time? What was done at that time? Signature of patient, parent, or guardian _____ date _____ although dental personnel. Medical and dental history patient name: I understand that providing incorrect information can be dangerous to my (or patient's) health. It is my responsibility to inform the dental office of any changes in medical status. I understand that providing incorrect information can be dangerous to my (or patient's) health. Date of your last dental exam: This form collects essential dental and medical history for patients. Complete this form accurately for. It ensures your dental professionals have the necessary information for treatment. A medical history form is a means to provide the doctor your health history. Please fill out this form completely so we can best care for you. How would you describe your current dental problem? 88 if child, mother’s history of decay? All information is strictly private and is protected. What was done at that time? Use the 2021 edition of the ada patient dental and medical health history information form to collect pertinent health information and history from your patients before treatment. Sample health history forms are available through the american dental association’s (ada) department of product development and sales and can be ordered online. Signature of patient, parent,. I understand that providing incorrect information can be dangerous to my (or patient's) health. Are you now under the care of a. Use this online form to collect dental medical history information from your patients. Our goal is to help you reach and maintain optimal oral health. 90 family history of periodontal disease? Complete this form accurately for. The american dental association (ada) offers a comprehensive health history form, for adults or children in both english and spanish, that covers both medical and dental issues. Use this online form to collect dental medical history information from your patients. 90 family history of periodontal disease? Our goal is to help you reach and maintain. All information is completely confidential. Use this online form to collect dental medical history information from your patients. Are you now under the care of a. 89 treatment for periodontal (gum) disease? I understand that providing incorrect information can be dangerous to my (or patient's) health. Use the 2021 edition of the ada patient dental and medical health history information form to collect pertinent health information and history from your patients before treatment. Have you had a serious/difficult problem associated with any previous dental treatment? This form collects essential dental and medical history for patients. To the best of my knowledge, the questions on this form. Sample health history forms are available through the american dental association’s (ada) department of product development and sales and can be ordered online. To the best of my knowledge, the questions on this form have been accurately answered. 90 family history of periodontal disease? Your response to indicate if you have or have not had any of the following diseases. All information is completely confidential. Download free medical history form samples and templates. Have you had a serious/difficult problem associated with any previous dental treatment? It is my responsibility to inform the dental office of any changes in medical status. Your response to indicate if you have or have not had any of the following diseases or problems. 89 treatment for periodontal (gum) disease? All information is completely confidential. To the best of my knowledge, the questions on this form have been accurately answered. Have you had a serious/difficult problem associated with any previous dental treatment? A medical history form is a means to provide the doctor your health history. How would you describe your current dental problem? The american dental association (ada) offers a comprehensive health history form, for adults or children in both english and spanish, that covers both medical and dental issues. Your response to indicate if you have or have not had any of the following diseases or problems. Please complete both sides of this dental/medical. It ensures your dental professionals have the necessary information for treatment. Current dental terminology © 2020 american dental association. Signature of patient, parent, or guardian _____ date _____ although dental personnel. Sample health history forms are available through the american dental association’s (ada) department of product development and sales and can be ordered online. Your response to indicate if you. This form collects essential dental and medical history for patients. This form provides a detailed overview of a patient's medical history, including a patient's dental history, previous dental treatments, specific medical conditions they might. Use this online form to collect dental medical history information from your patients. Your response to indicate if you have or have not had any of the following diseases or problems. All information is strictly private and is protected. Signature of patient, parent, or guardian _____ date _____ although dental personnel. Dental medical and history update to ensure the highest quality of healthcare, we ask that you complete this patient update form. Have you had a serious/difficult problem associated with any previous dental treatment? A medical history form is a means to provide the doctor your health history. What was done at that time? What was done at that time? The american dental association (ada) offers a comprehensive health history form, for adults or children in both english and spanish, that covers both medical and dental issues. Please complete both sides of this dental/medical history form so that we may provide you with the best possible dental care. Current dental terminology © 2020 american dental association. 89 treatment for periodontal (gum) disease? Our goal is to help you reach and maintain optimal oral health.
MEDICALHISTORYFORMENGLISHMedicalCenter1 ABC Dental
Medical History Forms 10 Free PDF Printables Printablee
Patient Medical Dental History printable pdf download
Printable Medical History Form For Dental Office
Printable Dental Health History Form
Printable Dental Medical History Form Template Printable Templates
Printable Medical History Form For Dental Office

Medical History Forms 10 Free PDF Printables Printablee
Printable Medical History Form For Dental Office

Printable Medical History Form For Dental Office Printable Word Searches
It Ensures Your Dental Professionals Have The Necessary Information For Treatment.
Use The 2021 Edition Of The Ada Patient Dental And Medical Health History Information Form To Collect Pertinent Health Information And History From Your Patients Before Treatment.
Are Any Of Your Teeth.
Sections For Contact Information, Prior Cleanings, And Medical.
Related Post: